ECG EXAMPLE #6
SCROLL DOWN FOR INTERPRETATION AND HISTORY
|
|
|
ECG #6 (12-lead ECG)
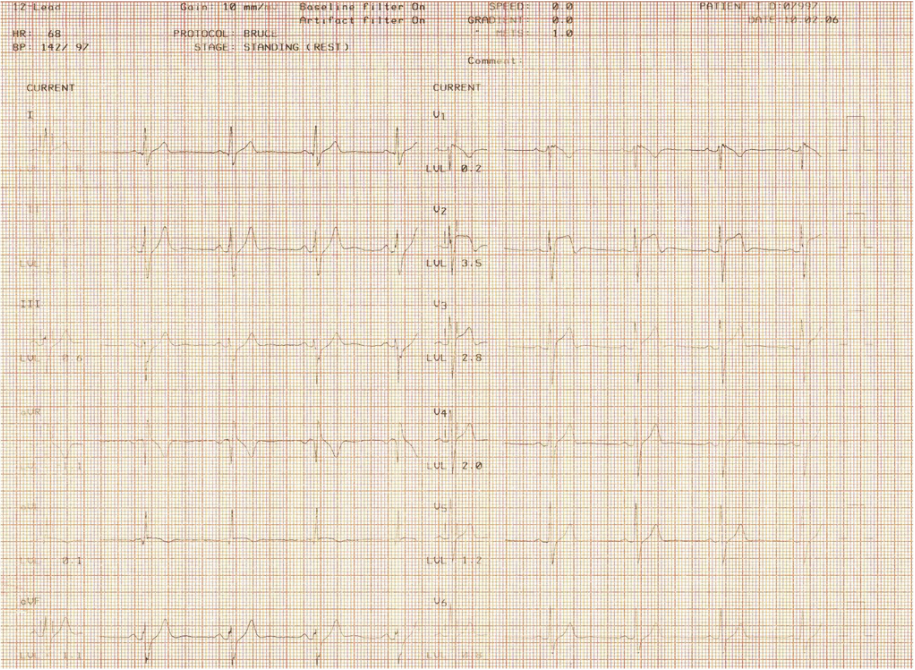
The patient was an asymptomatic 46 year old male referred for a treadmill exercise test. His ECG shows an atypical right bundle branch block pattern with a very high ST takeoff (>3mm in V2) in the right praecordial leads V1 to V3, with T wave inversion in V1 & V2. This is an example of Brugada Syndrome which was first described in 1992. The diagnosis is made on the ECG abnormality (this may vary significantly from time to time in individual patients) which occurs in the absence of structural heart disease or ischaemia. Its importance lies in its association with sudden unexplained death syndrome (SUDS) in individuals <40 years of age and it is particularly common in Southeast Asia. Patients may present with syncope due to polymorphic VT or resuscitated sudden death. In adults there is a 4:1 M:F preponderance.
The patient was an asymptomatic 46 year old male referred for a treadmill exercise test. His ECG shows an atypical right bundle branch block pattern with a very high ST takeoff (>3mm in V2) in the right praecordial leads V1 to V3, with T wave inversion in V1 & V2. This is an example of Brugada Syndrome which was first described in 1992. The diagnosis is made on the ECG abnormality (this may vary significantly from time to time in individual patients) which occurs in the absence of structural heart disease or ischaemia. Its importance lies in its association with sudden unexplained death syndrome (SUDS) in individuals <40 years of age and it is particularly common in Southeast Asia. Patients may present with syncope due to polymorphic VT or resuscitated sudden death. In adults there is a 4:1 M:F preponderance.