ECG EXAMPLE #8
SCROLL DOWN FOR INTERPRETATION AND HISTORY
|
|
|
ECG #8 (12 lead ECG)
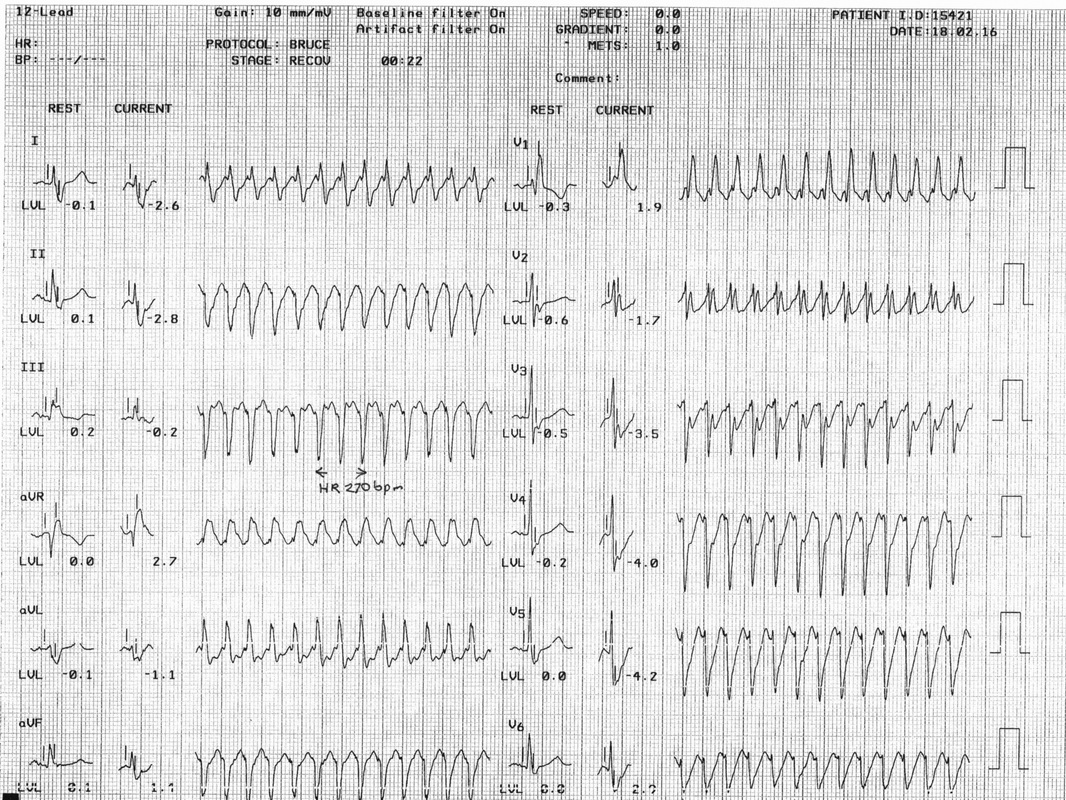
The patient was a 70 year old male with several risk factors for coronary artery disease referred for a treadmill exercise test because of recent episodes of palpitations.
At 8:30 minutes on the Bruce Protocol the patient abruptly developed a very rapid broad-complex tachycardia with heart rate quickly climbing to 270bpm. The tachycardia showed right bundle branch block morphology and left axis deviation consistent with left anterior hemiblock.
Superficially the ECG appearance suggests ventricular tachycardia but the patient had pre-existing right bundle branch block (with LAHB) and carotid sinus massage approximately halved the heart rate with the ECG briefly showing atrial flutter with 2:1 AV conduction before rapidly converting to atrial fibrillation with a rapid ventricular response.
The ECG therefore shows atrial flutter with 1:1 AV conduction. Such an occurrence is (thankfully) very rare but may be seen in patients on amiodarone in which the flutter waves may broaden with the atrial rate slowing to around 140 per minute instead of the usually 250-350 per minute.
In untreated atrial flutter patients seen often have 2:1 AV conduction during waking hours generally with variable block or 4:1 AV conduction during sleep.
The patient was a 70 year old male with several risk factors for coronary artery disease referred for a treadmill exercise test because of recent episodes of palpitations.
At 8:30 minutes on the Bruce Protocol the patient abruptly developed a very rapid broad-complex tachycardia with heart rate quickly climbing to 270bpm. The tachycardia showed right bundle branch block morphology and left axis deviation consistent with left anterior hemiblock.
Superficially the ECG appearance suggests ventricular tachycardia but the patient had pre-existing right bundle branch block (with LAHB) and carotid sinus massage approximately halved the heart rate with the ECG briefly showing atrial flutter with 2:1 AV conduction before rapidly converting to atrial fibrillation with a rapid ventricular response.
The ECG therefore shows atrial flutter with 1:1 AV conduction. Such an occurrence is (thankfully) very rare but may be seen in patients on amiodarone in which the flutter waves may broaden with the atrial rate slowing to around 140 per minute instead of the usually 250-350 per minute.
In untreated atrial flutter patients seen often have 2:1 AV conduction during waking hours generally with variable block or 4:1 AV conduction during sleep.